How Do I Know If I Need B12 Injections B12 Shots in Friso, Sherman, Anna. and Sunnyvale, TX
Introduction
If you’ve been wondering how do i know if i need b12 injections, you’re not alone—especially when symptoms like fatigue, tingling, or brain fog show up but your lab results are unclear or inconsistent. In my hands-on work with patients in clinics across the U.S., I’ve learned that the real challenge isn’t “Do I feel tired?” It’s figuring out which deficiency pattern you might have, whether B12 injections are clinically appropriate, and what to rule out before starting treatment.
This guide focuses on what I look for when someone asks about B12 shots—whether you’re in Frisco, Sherman, Anna, or Sunnyvale, TX—or anywhere else. You’ll learn how clinicians decide if B12 injections make sense, what tests matter, and when oral therapy or other causes should be prioritized instead.
First: What B12 injections are (and what they are not)
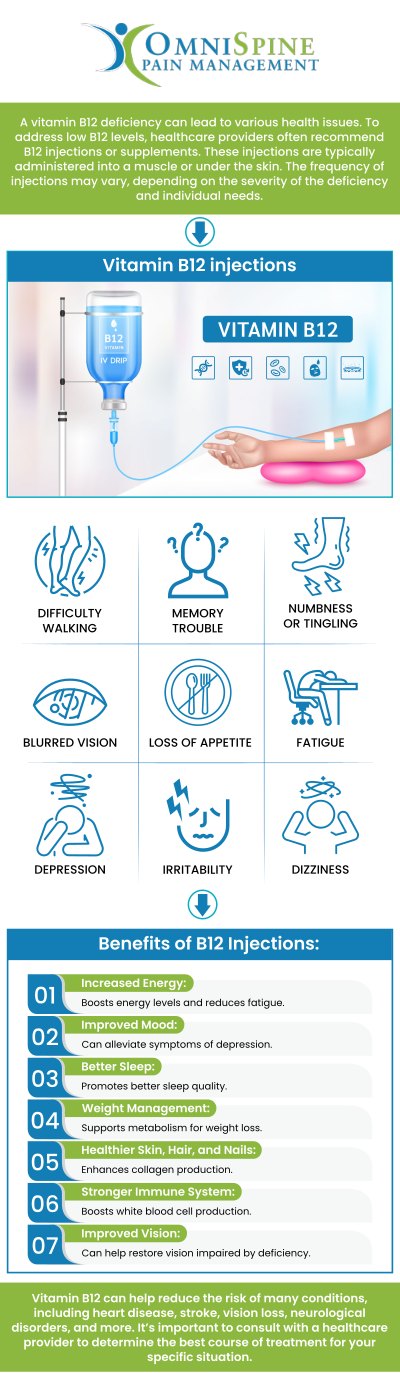
Vitamin B12 injections are a medical approach to correcting low B12 levels. The goal is to replenish your B12 stores quickly and sustainably, especially when absorption from food or oral supplements is impaired.
In practice, B12 injections are most likely to be recommended when:
- Your B12 level is low (based on lab testing), especially if symptoms are present.
- You have a reason B12 won’t absorb well (examples include pernicious anemia, certain stomach or intestinal conditions, or specific medication effects).
- You have neurologic symptoms (like tingling/numbness, balance issues), where prompt correction is important.
What they are not: a general-purpose energy booster for everyone. In my experience, many people feel better only when the underlying cause is addressed—not just when a shot is given.
How do i know if i need b12 injections? Key signs clinicians look for
When someone asks how do i know if i need b12 injections, I start with a symptom-to-mechanism check. B12 deficiency can affect red blood cells and the nervous system. That’s why symptoms cluster into a few patterns.
Common symptoms that can fit B12 deficiency
- Fatigue and low stamina
- Shortness of breath with exertion (sometimes from anemia)
- Glossitis (sore, smooth tongue)
- Neurologic symptoms: numbness/tingling, “pins and needles,” balance problems, memory or concentration issues
Red flags that should speed up evaluation
- Progressive numbness or weakness
- Gait changes or frequent stumbling
- Severe anemia signs (such as marked exercise intolerance)
These don’t automatically mean “you need injections,” but they raise the priority for getting the right tests quickly.
Risk factors that make B12 injections more likely to be appropriate
In real-world care, risk factors often determine whether injections are a faster, more reliable route than oral B12. I’ve seen this especially with patients who:
- Have pernicious anemia or autoimmune gastritis
- Have had gastric or intestinal surgery (or chronic malabsorption issues)
- Take medications that can impair absorption (for example, long-term acid suppression in some cases)
- Follow diets with limited B12 intake (higher risk if diet is very restricted)
- Have conditions affecting the ileum (where B12 absorption occurs)
The tests that actually answer the question
If you’re trying to decide how do i know if i need b12 injections, lab testing is what turns a guess into a plan. In my hands-on approach, I favor testing that doesn’t just show “low” or “normal,” but clarifies whether B12 deficiency is functionally present.
1) Serum B12 (a starting point)
This is often the first test ordered. However, serum B12 can sometimes be “borderline,” which is where clinicians may look for additional markers.
2) Methylmalonic acid (MMA) and/or homocysteine
These help detect functional deficiency. When B12 is insufficient at the tissue level, MMA and homocysteine may rise. In practice, these tests are especially useful when symptoms exist but serum B12 isn’t clearly low.
3) Complete blood count (CBC) and sometimes folate
A CBC can show anemia patterns that fit B12 deficiency. Folate is relevant too, because deficiency patterns can overlap—plus treatment strategy can change depending on what else is going on.
4) If pernicious anemia is suspected
Additional evaluation may include tests for autoimmune causes of impaired absorption (your clinician will decide what’s appropriate based on history and symptoms).
My practical takeaway: the “best” test set depends on your risk factors and symptom profile. But if you’re asking about B12 injections, you generally want data that explains why your level is low or borderline—not just a single number.
B12 injections vs oral B12: how to decide what makes sense
Not every patient with low or borderline B12 needs injections. In many cases, oral supplementation can work—especially when absorption is intact. But when absorption is impaired, injections are often the more dependable option.
When injections are commonly favored
- Clear deficiency with neurologic symptoms
- Suspected or confirmed malabsorption (e.g., pernicious anemia)
- Need for faster correction in symptomatic patients
When oral therapy may be reasonable
- Mild deficiency without neurologic symptoms
- Dietary insufficiency with otherwise normal absorption
- Patient preference and ability to adhere to an oral plan
A real-world “lesson learned” from my clinic experience
One recurring pattern: a patient gets an injection “because they’re tired,” but their fatigue is driven by something else—sleep apnea, thyroid issues, iron deficiency, stress, or medication effects. I’ve also seen people improve only after we address the real cause (not the B12). That’s why in my workflow I try to connect symptoms to a defensible B12 deficiency mechanism, and I use labs to guide whether injections are warranted.
What the injection plan typically considers (dose, frequency, and monitoring)
There isn’t one universal schedule for everyone. Clinicians tailor treatment based on baseline levels, symptoms, underlying cause, and response. In my experience, the best plans include monitoring rather than assuming the shot “solves everything.”
Factors that influence a B12 injection plan
- Your starting B12 status (and sometimes MMA/homocysteine)
- Presence and severity of neurologic symptoms
- Cause (dietary vs malabsorption-related)
- Whether anemia is present
- Response over time (symptoms and follow-up labs)
Monitoring: what to expect
Monitoring often focuses on symptom improvement and normalization (or improvement) of relevant labs. If symptoms don’t improve as expected, it’s a signal to reassess the diagnosis and look for alternative causes.
When to avoid self-starting B12 injections
I recommend against starting injections purely based on internet symptom checklists. While B12 is generally considered well-tolerated for many patients, the real risk is missing the actual cause of symptoms. If you have significant neurologic symptoms, unexplained anemia, or rapidly worsening fatigue, you should get a clinical evaluation and appropriate labs rather than relying on trial-and-error.
FAQ
What symptoms mean I might need B12 injections?
Symptoms that can fit B12 deficiency include fatigue, anemia-related shortness of breath, sore/smooth tongue, and neurologic signs like numbness or tingling. If you have neurologic symptoms, evaluation should be prioritized, and labs such as serum B12 plus MMA and/or homocysteine are often considered.
Can I tell I need injections without tests?
Not reliably. You might have risk factors that make deficiency more likely, but determining whether injections are appropriate generally requires labs and clinical context. “Borderline” results are especially where follow-up markers (like MMA/homocysteine) can clarify the picture.
If my B12 is normal, should I still get injections?
A normal serum B12 reduces the likelihood of true B12 deficiency, but it doesn’t always answer the question if symptoms and risk factors suggest functional deficiency. In those cases, clinicians may consider additional tests and look for other causes of symptoms instead of assuming B12 injections are the solution.
Conclusion
So, how do i know if i need b12 injections? The strongest answer is: you look at your risk factors, symptom pattern (especially neurologic symptoms), and confirm with appropriate lab testing that explains whether you truly have B12 deficiency—and why.
Next step: Schedule a clinical evaluation and ask for a lab plan tailored to your symptoms and risk factors (often including serum B12 and, when appropriate, MMA and/or homocysteine). That’s the point where treatment decisions become grounded in evidence instead of guesswork.
Discussion