Are Vitamin B12 Shots Right for You?
Are Vitamin B12 Shots Right for You?
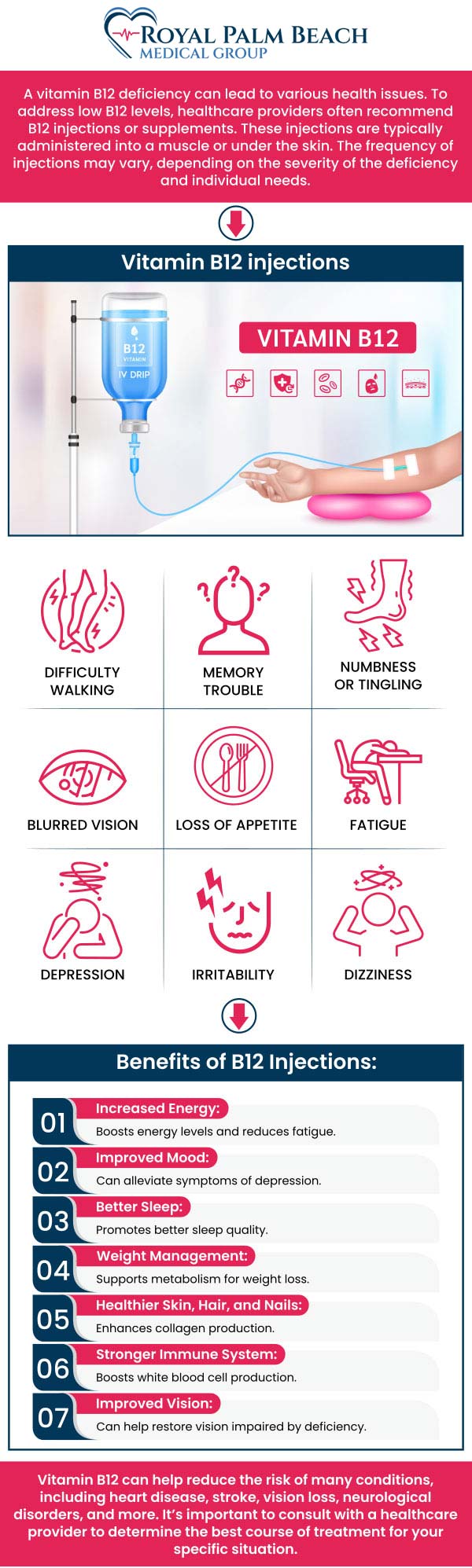
If you’ve ever felt tired all the time, noticed tingling or numbness in your hands or feet, or just struggled to make it through the day, you may have wondered whether you’re dealing with a vitamin B12 deficiency. In my hands-on clinic work, I’ve seen people try “general” supplements that didn’t move the needle—only to get clearer answers once we looked at why B12 was low and when to get B12 injections instead of guessing.
This article breaks down when B12 shots make sense, when they don’t, and how to decide based on symptoms, labs, and the underlying cause. If you’re considering injections, you’ll leave with a practical framework you can use to talk with a clinician and make an informed plan.
What B12 Injections Actually Do (and Why Timing Matters)
Vitamin B12 injections deliver cobalamin directly into the body, bypassing some absorption issues that can prevent oral supplements from working well. The goal isn’t just “to raise numbers”—it’s to restore healthy red blood cell production, support neurological function, and correct the specific deficiency mechanism that caused low B12 in the first place.
In practice, timing matters because B12 deficiency can develop and progress differently depending on the cause:
- Rapid symptom relief is not always immediate. People often feel better after a few weeks when labs and symptoms respond, but neurological symptoms (tingling, numbness) may take longer.
- Underlying causes determine whether injections are short-term or long-term. If there’s a malabsorption condition, injections may be needed to maintain adequate levels.
- Starting sooner can reduce risk of persistent nerve changes. The longer deficiency goes untreated, the more likely symptoms can linger.
That’s why the decision is not only “shots vs pills,” but also when to get B12 injections relative to your lab results, symptom severity, and diagnosis.
When to Get B12 Injections: Common Scenarios
In my experience reviewing cases across primary care and chronic care settings, B12 shots are most compelling when deficiency is confirmed and there’s a reason oral therapy is unlikely to work—or when symptoms suggest the body needs faster replenishment.
1) You have confirmed deficiency and suspected malabsorption
Oral B12 may fail when absorption is impaired. Clinicians commonly consider injections if the cause includes:
- pernicious anemia (autoimmune-related intrinsic factor deficiency)
- post-gastric surgery states (bypass or removal affecting absorption)
- inflammatory bowel disease or other GI disorders affecting absorption
- chronic GI conditions leading to low intrinsic factor or poor uptake
Why this works: injections reduce reliance on gut absorption pathways, helping you reach therapeutic B12 levels even when the GI tract isn’t cooperating.
2) Neurological symptoms are present
If you have neurological concerns such as numbness, tingling, balance issues, or cognitive changes tied to low B12, many clinicians lean toward injections sooner rather than later.
In my hands-on work: I’ve seen patients who were “just tired” for months develop clear nerve-related symptoms after they stopped follow-up labs. The key lesson was that once neuro symptoms appear, delaying treatment can mean slower or incomplete recovery.
3) Lab results show significant deficiency
Deficiency severity matters. If bloodwork confirms low B12 and clinicians suspect functional deficiency, injections are often used to correct the deficit more predictably.
Often, clinicians don’t rely on B12 alone—they may also check markers such as methylmalonic acid (MMA) and homocysteine to better assess tissue-level deficiency.
4) Oral therapy hasn’t worked (or adherence is a problem)
Some people simply can’t maintain an oral regimen, or they don’t respond despite taking supplements correctly. If levels remain low, injections can be a practical next step.
Important limitation: injections aren’t a cure for the cause. If malabsorption continues, you may need ongoing treatment or a maintenance strategy.
When B12 Shots May Not Be the Best First Step
B12 injections are not automatically the right move for everyone. In several real-world situations, oral supplementation and addressing diet or medication factors can be sufficient—especially when deficiency is mild, symptomatic issues are limited, and malabsorption is unlikely.
1) Your deficiency is mild and oral therapy is appropriate
If a clinician believes absorption is intact, higher-dose oral B12 can sometimes raise levels effectively. In those cases, injections may not add much beyond convenience.
2) Your symptoms have other likely explanations
Fatigue and tingling can stem from iron deficiency, thyroid disease, vitamin B6 issues, diabetes or neuropathy, sleep apnea, medication side effects, and more. Treating “just B12” without evaluating alternatives can lead to months of frustration.
My practical rule: when symptoms are non-specific, we look for pattern + labs together. Non-specific symptoms alone weren’t enough to justify injections in my earlier years, and that approach changed how quickly we solved problems.
3) There’s no confirmed deficiency
If your B12 is normal and you’re considering injections because of general wellness marketing, it’s usually better to focus on nutrition, risk factors, and evidence-based testing.
How Clinicians Typically Structure Treatment (What to Expect)
Treatment plans vary based on diagnosis, severity, and response. Here’s the practical concept most clinicians follow:
- Correction phase: injections are given on a schedule to restore B12 levels.
- Repletion and monitoring: clinicians reassess symptoms and often repeat labs to confirm response.
- Maintenance phase: if the cause persists, injections may continue at intervals; if reversible, a maintenance plan may switch to oral therapy.
What I recommend you ask for: your target labs, the timeline for re-checking, and the plan if symptoms don’t improve as expected.
Risks, Side Effects, and Practical Considerations
B12 injections are generally well-tolerated, but side effects can occur. In real clinical settings, common issues include soreness at the injection site, mild headache, or nausea. More serious reactions are uncommon but possible, especially in people with sensitivities to components in the formulation.
Also consider these practical points:
- Don’t skip follow-up labs. If you feel no improvement, it may mean the cause isn’t B12—or that another deficiency or condition needs attention.
- Maintenance matters. If malabsorption or pernicious anemia is the cause, stopping treatment can lead to recurrence.
- Neurological symptoms can be slower to recover. The goal is stabilization and gradual improvement; early treatment often helps outcomes.
How to Decide: A Simple, Evidence-Based Checklist
If you’re trying to determine whether you should get injections, use this decision framework:
- Have you tested? Ask about B12 and, if appropriate, MMA/homocysteine.
- Do you have risk factors? Pernicious anemia, GI surgery, chronic GI disease, long-term acid suppression, vegan/vegetarian diet without supplementation.
- Are symptoms neurological? Tingling, numbness, balance issues, cognitive changes.
- Has oral treatment worked? If it hasn’t, injections can be a logical step.
- Do you have a plan for maintenance? “Short course” only works when the cause is reversible.
This checklist helps you align treatment with the underlying mechanism—one of the biggest factors in whether people feel better and stay better.
FAQ
How soon should I get B12 injections if I think I’m deficient?
If you have confirmed low B12 (especially with neurological symptoms), it’s reasonable to discuss injections promptly with a clinician rather than waiting. The exact timing depends on your diagnosis and severity, but delaying follow-up after symptoms begin is a common reason people don’t improve as expected.
When to get B12 injections versus taking oral B12?
Clinicians often favor injections when malabsorption is likely (e.g., pernicious anemia or post-bariatric surgery), when labs suggest significant deficiency, when neurological symptoms are present, or when oral therapy hasn’t corrected levels. Oral B12 may be sufficient when absorption is expected to be intact and deficiency is mild.
Will B12 shots fix fatigue right away?
Not always. Fatigue can improve after B12 levels normalize, but the timeline varies. In my experience, improvement is more likely when labs confirm deficiency and when other causes (iron deficiency, thyroid issues, sleep problems, medication effects) are addressed at the same time.
Conclusion
Are Vitamin B12 shots right for you? They’re most effective when B12 deficiency is confirmed and the underlying cause suggests injections will overcome absorption problems or address neurological risk. The best decisions come from matching treatment to your diagnosis—so the real question is not only “shots vs pills,” but when to get B12 injections based on labs, symptoms, and the mechanism behind low B12.
Next step: book an appointment and ask for B12 testing (and, if needed, MMA/homocysteine), plus a clear plan for treatment and follow-up labs based on your results and symptom pattern.
Discussion